

Yale research confirms Borrelia miyamotoi causing infection in US
A tickborne disease caused by spirochetes more closely related to relapsing fever spirochetes than Lyme disease spirochetes was found in 18 patients in southern New England and New York, according to research published in the New England Journal of Medicine January 17.
The infection - caused by spirochetal bacteria known as Borrelia miyamotoi - was detected in 21 percent of 14 patients with unexplained summertime febrile illness, 3 percent of 273 patients with Lyme disease (or suspected Lyme disease), and 1 percent of 584 healthy people from areas endemic for Lyme disease.
This study is one of a few which offer the indication that infection with Borrelia miyamotoi in North America is less common than its well-known more distantly related relative, Borrelia burgdorferi, the spirochete which causes Lyme disease.
It's estimated 2-3,000 people* in the United States may be infected with Borrelia miyamotoi annually - but due to it being an emerging infectious disease which is difficult to diagnose, how common it is and will be in the future remains to be seen.
In surveillance studies, anywhere from 1-16% of Ixodes scapularis ticks have been infected with Borrelia miyamotoi, depending on the region. This is about the same percentage range of Ixodes ticks which are infected with Borrelia miyamotoi in Russia and Western Europe.
In North America, Ixodes ticks infected with Borrelia miyamotoi have been found in the northeastern US, midwest, west coast, and Canada.
How Borrelia miyamotoi infection differs from Lyme disease
Early symptoms
Clinically speaking, an infection with B. miyamotoi has symptoms which overlap those of Lyme disease. They include fever, muscular aches and pains, joint aches, chills, sweats, vomiting (sometimes), headaches and fatigue, with a small portion also developing a rash such as with Lyme disease. Also, symptoms can be more severe than those found in Lyme disease and some patients may require treatment in a hospital.
The two most striking differences between B. miyamotoi infections and Lyme disease?
Usually there isn't a rash - the exact opposite of Lyme disease. One Russian study stated that more than 50% of patients documented with the disease did not have a characteristic rash. According to Dr. Peter Krause, only 10-15% of patients get a rash and it is usually smaller than those seen in Lyme disease.
Sometimes, people get cycling, spiking fevers. Studies demonstrated that some patients had episodes of high spiking fevers which occurred days or one to two weeks apart. These cyclical fevers and the lack of a rash map closely to symptoms found in relapsing fever - a spirochetal disease which is usually transmitted by soft-bodied ticks.
Here is an example of two patterns of fever and symptoms found in patients studied in Russia [pdf]:
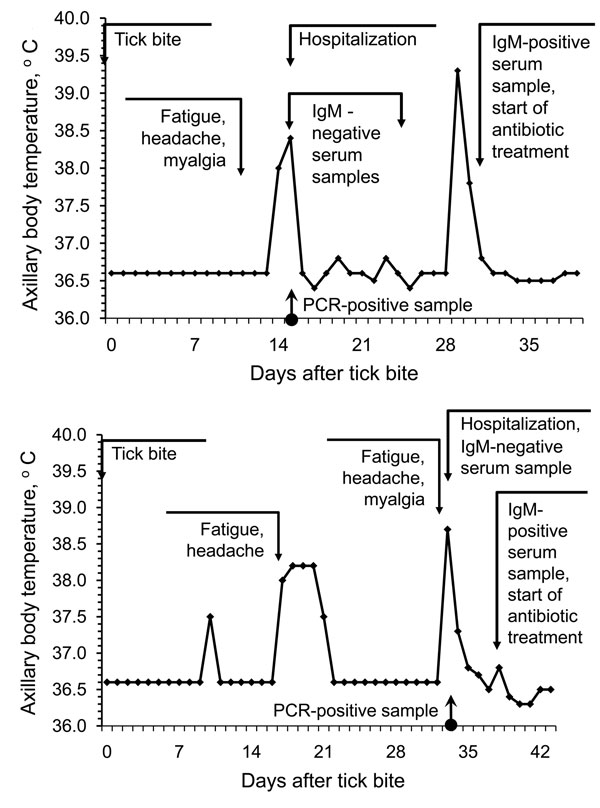 |
| Graph From: Humans Infected with Relapsing Fever Spirochete Borrelia miyamotoi, Russia Emerg Infect Dis. 2011;17:1816-1823 |
Later stages of infection
Not much is known about later stages of infection with B. miyamotoi. This is because its study in human and animal hosts is relatively new, having been discovered only in 1995 in Japan.
However, one could potentially extrapolate how B. miyamotoi will behave after initial infection by looking at research on its genetically closest living relatives which are also relapsing fever spirochetes.
Borrelia miyamotoi's closest living relatives appear to be Borrelia hermsii and Borrelia lonestari.

Image from: Typing of Borrelia Relapsing Fever Group Strains.
Emerg Infect Dis. 2004 September; 10(9): 1661–1664.
doi: 10.3201/eid1009.040236
Testing for the presence of Borrelia miyamotoi
From both the patient's and the doctor's point of view, one troubling aspect of being infected with Borrelia miyamotoi is that even if the patient has a history of a tick bite and has symptoms which seem similar to those found in Lyme disease - a blood test for Lyme disease will be negative.
This is because Borrelia miyamotoi is genetically distant enough from Borrelia burgdorferi that the antibodies produced in response to miyamotoi seldom cross react with those of Borrelia burgdorferi.
So how do you test for the presence of Borrelia miyamotoi?
If you're a microbiologist and do not have access to antibody testing, have an acutely ill patient in front of you with a current flare up of symptoms including spiking fever, a blood smear and dark field microscopy might yield a positive result for Borrelia miyamotoi - as it does for other relapsing fever spirochetes.
But most family physicians will likely want to order a blood test using PCR and/or an antibody test specifically designed for relapsing fever in order to detect infection.
In a study of 47 Russian patients found to have infections with Borrelia miyamotoi, presence of infection could be detected using an ELISA (EUROIMMUN AG, Lübeck, Germany) for major Borrelia burgdorferi sensu latu genospecies found in Europe - but it could not discriminate (sort) specific antibodies against any of these species.
Given that ELISA tests for Borrelia other than Borrelia burgdorferi sensu strictu are hard to come by in the US and Canada, the detection of Borrelia miyamotoi using standard Lyme disease ELISA may not work in North America.
Instead of a standard North American Lyme disease ELISA or EUROIMMUN AG, an ELISA or Western Blot for relapsing fever which contains GlpQ protein - an antigen which is non-reactive to Borrelia burgdorferi antibody - can be used to detect infection with Borrelia miyamotoi.
This information should serve as a cautionary tale for the doctor:
If a patient has been in an environment where ticks are found and has Lyme disease-like symptoms or a summer flu, consider relapsing fever as a differential diagnosis - especially if the patient does not recover as they would from a flu and has a negative Lyme disease ELISA.
Blood tests and PCR are most likely to yield a positive result when a sample is taken during a patient's spiking fever and the height of symptoms because that is when spirochetemia is peaking. With each relapse of infection, the number of spirochetes in the blood is reduced - thus making it less likely to obtain positive test results the later it is during the course of infection.
Treatment
So far, all the research points to the same antibiotics being used for Lyme disease as being effective for treating relapsing fever, and this extends to infections with Borrelia miyamotoi. In addition to amoxicillin, tetracycline, and doxycycline, relapsing fever has also been treated with chloramphenicol with success. Intravenous ceftriaxone may be required for more severe illness.
If a patient with Borrelia miyamotoi is treated with antibiotics and continues to suffer from high spiking fevers and other symptoms, retreatment may be needed with intravenous antibiotics. Co-infections such as babesiosis and ehrlichiosis should be investigated as they can produce similar symptoms.
In a 2011 study on Russian patients treated for Borrelia miyamotoi infection, this was the treatment and outcome:
Therapy consisted of ceftriaxone, 2 g intravenously every 24 hours for 2 weeks (42 patients) or doxycycline 100 mg orally every 12 hours for 2 weeks (2 patients). Two patients received no antimicrobial drug while hospitalized; 1 later received doxycycline at home, and the other was readmitted to the hospital for relapse and received ceftriaxone.
Outcome
Some relapsing fever strains can cause severe illness, and without treatment these strains have a high rate of case fatality. So far, B. miyamotoi lies along a spectrum of illness which appears to range from mild to moderate severity, but even so, infection should be treated with antibiotics immediately to avoid complications.
The good news is that most people who are infected with relapsing fever and are treated promptly with antibiotics go on to recover. The same will probably apply to infection with B. miyamotoi based on research published to date - but the true picture remains uncertain until more patients are diagnosed, treated, and proper follow-up is completed.
Complications
Are the complications found in Borrelia miyamotoi infections going to be the same as those found in Lyme disease? Given that it is genetically closer to relapsing fever spirochetes and more distant to Borrelia burgdorferi, one could speculate that it may have characteristics and complications common to relapsing fever - but without further research, it is unclear.
The risk for infected untreated pregnant women to pass on infection to the fetus in utero with a negative outcome (e.g. miscarriage; defects) might be more likely than it is in Lyme disease. Infection of the central nervous system may also occur more rapidly than it typically does in Lyme disease. But this is speculative, due to being based on research where there is variability in severity and outcome across relapsing fever strains.
Facts and uncertainties
It is known that in many cases, Borrelia miyamotoi - unlike Borrelia burgdorferi - is transmitted transovarially in deer ticks. This means the female tick infects her offspring, which produces infected larvae. These larvae will go on to molt and become infected nymphs. (Transovarial infection is rare to nonexistent in Borrelia burgdorferi.)
It is also known that relapsing fever spirochetes in soft-bodied ticks reside in tissues throughout the tick - whereas Lyme disease spirochetes are only found in the midgut.
Thus a significant question arises: What role does a relapsing fever spirochete play in relation to its hard-bodied tick host, and how soon can a tick transmit infection with Borrelia miyamotoi after attachment? This appears to be unknown.
Other questions based on how other relapsing fever strains also present themselves: How neurotropic is Borrelia miyamotoi? Can it become a latent infection, as was discovered in other relapsing fever strains? How rapidly does it differentiate into different serotypes found in different tissues?
The answers to these questions - and more - are also unknowns until this bacteria is studied more carefully. Similar questions may also arise in research on Borrelia lonestari in Amblyomma americanum ticks - another relapsing fever type spirochete found in a hard-bodied tick.
* Jan 19, 2013 Edited to add: Dr. Peter Krause offered a more recent estimate of 3-4,000 cases of B. miyamotoi occur in US annually.
Image Credit: Photography by Alan R. Walker, of Borrelia theileri infecting the blood plasma of a cow. Giemsa stained. Borrelia theileri is closely related to both B. lonestari and B. miyamotoi, and causes bovine Borreliosis in cattle. Source: http://commons.wikimedia.org/wiki/File:Borrelia-theileri-cow.jpg
References
Human Borrelia miyamotoi Infection in the United States
N Engl J Med 2013; 368:291-293 January 17, 2013 DOI: 10.1056/NEJMc1215469 http://www.nejm.org/doi/full/10.1056/NEJMc1215469
Carl-Johan Fraenkel, Ulf Garpmo,Johan Berglund. Determination of Novel Borrelia Genospecies in Swedish Ixodes ricinus Ticks. J. Clin. Microbiol. September 2002 ; 40:9 3308-3312 doi:10.1128/JCM.40.9.3308-3312.2002 http://jcm.asm.org/content/40/9/3308.full
Rebaudet, Stanislas, and Philippe Parola. Epidemiology of relapsing fever borreliosis in Europe. FEMS Immunology & Medical Microbiology 48.1 (2006): 11-15. http://onlinelibrary.wiley.com/doi/10.1111/j.1574-695X.2006.00104.x/full
Sarah A Hamer, Graham J Hickling, Rich Keith, Jennifer L Sidge, Edward D Walker, and Jean I Tsao. Associations of passerine birds, rabbits, and ticks with Borrelia miyamotoi and Borrelia andersonii in Michigan, U.S.A. Parasit Vectors. 2012; 5: 231.
Published online 2012 October 11. doi: 10.1186/1756-3305-5-231 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3497883/
Scott, M. C., et al. High-Prevalence Borrelia miyamotoi Infection Among Wild Turkeys (Meleagris gallopavo) in Tennessee. Journal of medical entomology 47.6 (2010): 1238-1242. http://www.bioone.org/doi/abs/10.1603/ME10075
Mun J, Eisen RJ, Eisen L, Lane RS. Detection of a Borrelia miyamotoi sensu lato relapsing-fever group spirochete from Ixodes pacificus in California.
http://www.ncbi.nlm.nih.gov/pubmed/16506458
Ogden, Nick H., et al. Investigation of genotypes of Borrelia burgdorferi in Ixodes scapularis ticks collected during surveillance in Canada. Applied and environmental microbiology 77.10 (2011): 3244-3254. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3126474/
Fukunaga M, Takahashi Y, Tsuruta Y, et al. Genetic and phenotypic analysis of Borrelia miyamotoi sp. nov., isolated from the ixodid tick Ixodes persulcatus, the vector for Lyme disease in Japan. Int J Syst Bacteriol 1995;45:804-810
http://ijs.sgmjournals.org/content/45/4/804.full.pdf
Jonas Bunikis, Jean Tsao, Ulf Garpmo, Johan Berglund, Durland Fish, Alan G. Barbour.
Typing of Borrelia Relapsing Fever Group Strains. Emerg Infect Dis. 2004 September; 10(9): 1661–1664. doi: 10.3201/eid1009.040236 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3320305/
Scoles, Glen A., et al. A relapsing fever group spirochete transmitted by Ixodes scapularis ticks. Vector Borne and Zoonotic Diseases 1.1 (2001): 21-34. http://online.liebertpub.com/doi/abs/10.1089/153036601750137624
Tamar Halperina, Nadav Orrb, Regev Cohena, Tal Hasina, Nadav Davidovitchc, Eyal Klementa, Raid Kayoufa, Gad Banethd, Dani Cohenb, Miri Yavzoria. Detection of relapsing fever in human blood samples from Israel using PCR targeting the glycerophosphodiester phosphodiesterase (GlpQ) gene. Acta Tropica. Volume 98, Issue 2, May 2006, Pages 189–195 http://www.sciencedirect.com/science/article/pii/S0001706X0600074X
Schwan TG, Schrumpf ME, Hinnebusch BJ, Anderson DE Jr, Konkel ME. GlpQ: an antigen for serological discrimination between relapsing fever and Lyme borreliosis. J Clin Microbiol 1996;34:2483-2492 http://jcm.asm.org/content/34/10/2483.full.pdf
Karan' LS, Koliasnikova NM, Toporkova MG, Makhneva MA, Nadezhdina MV, Esaulkova AIu, Romanenko VV, Arumova EA, Platonov AE, Maleev VV. [Usage of real time polymerase chain reaction for diagnostics of different tick-borne infections]. [Article in Russian] Zh Mikrobiol Epidemiol Immunobiol. 2010 May-Jun;(3):72-7. http://www.ncbi.nlm.nih.gov/pubmed/20734723
Alan G. Barbour, Jonas Bunikis, Bridgit Travinsky, Anne Gatewood Hoen, Maria A. Diuk-Wasser, Durland Fish, and Jean I. Tsao. Niche Partitioning of Borrelia burgdorferi and Borrelia miyamotoi in the Same Tick Vector and Mammalian Reservoir Species. Am J Trop Med Hyg. 2009 December; 81(6): 1120–1131. doi:10.4269/ajtmh.2009.09-0208 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2841027/
Relapsing Fever. Columbia University Lyme and Tickborne Diseases Research Center. http://www.columbia-lyme.org/patients/tbd_relapsing.html
Researchers discover new tickborne infection. WTNH News 8. January 18, 2013 http://www.wtnh.com/dpp/news/health/researchers-discover-new-tick-borne-infection

This work by Camp Other is licensed under a Creative Commons
Attribution-NonCommercial-ShareAlike 3.0 Unported License.
